Treating Lung Patients with Hands Over Their Heads with Alpha Cradle® Forms
Sheila R. Polansky, RTRT
University of Texas Medical Branch
Galveston, Texas
The purpose of this paper will be to demonstrate the necessity of the ALPHA CRADLE® brand Patient Repositioning System, specifically, the head and shoulder 2 form, HS2, while resolving three specific problems. We encountered these problems while treating lung patients with their arms over their head.
The first of these problems deals with reproduction of the treatment field. When the arms are raised over the head, the back becomes rounded and the patient has a tendency to roll (if only slightly) on the treatment table. Then, also, if the patient becomes fatigued either during a lengthy simulation or a treatment day requiring port films, the arms start to relax thus changing set up points and treatment depths. These changes require frequent adjustments which add to the time the patient spends on the table. The ALPHA CRADLE® HS2, head & shoulder form, solved this problem perfectly! The patient fits right into the mold every time and also has a place to rest their arms so there is no movement.
The second problem we encountered, was that the elbows of some of our patients were too far apart to fit within the gantry radius of one of our high energy treatment machines. This was solved by raising the arms farther from the table, and moving the elbows medial. To do this we custom made armrests using Styrofoam® and lucite (Fig. 2) that are fastened to the HS2 form with Velcro® (Fig. 1). This raises the elbows a full 5 cm from the Alpha Cradle head & shoulder form (Fig. 6). Then by having the patient clasp their fingers, that brings the elbows medial just enough to fit within the gantry’s rotation.
Our third problem came when trying to simulate our elderly and post-surgical patients. These patients had difficulty putting their arms down into the form (Fig. 5). This problem was partially solved by the custom armrests. We then started using the AC325 foaming agent kit instead of the foaming agents included with the head & shoulder forms. We use those foaming agents for extremities and pediatric patients. By using the AC325 kit, it gave us twice as much foam to work with. By also using the bag included with this kit, we could force the foam under the shoulders and arms where these patients need the most support (Fig. 8).
At this point I would like to add that we have not found the need to cut out the posterior field. Most of the foaming agents are pushed upward when the patient lays down. We have also not noted an appreciable difference in skin reaction between anterior and posterior fields with regard to thickness of the cast.
In conclusion, I would like to say that since its inception at our facility, ALPHA CRADLE® forms have vastly improved reproduction in virtually all of our set ups.

Fig. 1 Form used for making the cradle.

Fig. 2 Custom armrests consisting of Styrofoam® blocks: 5 cm high, 3 cm wide, 12 cm long. Cups consist of a 12 cm long lucite tube 15 cm in diameter, cut across the diameter and covered in sponge tape.

Fig. 3 Placement of arm rests on the form.


Fig. 5 Shows placement of arms closer together with added stability by clasping the hands.

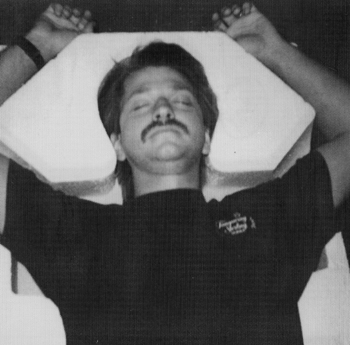
Fig. 6 Shows how far back the arms are putting strain on surgical scars and arthritic shoulders.

Fig. 7 Shows the arms in a higher relative position which is more comfortable.
DISCUSSION AND SUMMARY
Frolich3 in his discussion of radiation effects notes that cardiac radio-reactions can be transient or harmless and rarely can lead to acute left-threatening situation. However, long term morbidity from cardiac irradiation has been well documented. Radiation pericarditis and premature coronary artery disease have been described by Arsenian.4 Because significant curative therapeutic results can be obtained with radiotherapy in thoracic area and the chances for curing increase for many patients, a slight risk is justifiable for side effects on healthy adjoining tissue. On the other hand undesirable side reactions can influence the life-quality of the tumor cured patients, therefore, the aim of the radiation oncology team is to achieve uncomplicated local-regional control of cancer by radiation therapy. To accomplish this goal, precise knowledge of tumorcidal dosages and tolerance of doses of various normal tissues is most important. Unfortunately, after eight decades of radiotherapy practice, current knowledge of tolerance dose for healthy tissue an optimum curative dose for malignant tissues is still somewhat imprecise. In recent years, sophisticated treatment planning systems have been implemented. Actual CT images with the target and tumor volume superimposed with isodose curves representing the cumulative dosages of radiation to the tumor have aided in precision treatments. This advancement has resulted in major improvements to ensure adequate tumor coverage and better spacings of critical and normal structures. With the use of immobilization devices such as ALPHA CRADLE® brand Patient Repositioning Systems, positioning alternatives and treatments can be personalized under any circumstances. In this particular case the heart dose was reduced by 25% without compromising the dose to the lung tumor. It is our intention to use ALPHA CRADLE® forms on all patient procedures when a positioning variation is used.