ALPHA CRADLE BELLY BOARD FOR SMALL BOWEL MINIMIZATION
Lori E. Frank, RTTR, CMD
Laura A. Rowley, RTTR, CMD
Thomas G. Shanahan, MD
Minesh P. Mehta, MD
Univ. of Wisconsin Hospital & Clinics
Madison, Wisconsin
Many factors have been shown to affect the tolerance of the small bowel to external irradiation. Some examples are previous surgery, pelvic inflammatory disease, diabetes mellitus, hypertension, age, and the radiation variables of time, dose, and fractionation1,2,3,5,7,8. The occurrence of late complications may vary 2-30% in the first 18 months of follow-up because of the numerous factors affecting long term complications.
Both acute and late gastrointestinal side effects correlate with the volume of small bowel receiving 45 Gy or more with conventional treatment setups and fractionation; however, the exact extent of the relationship between volume treated and small bowel tolerance has not been determined1,4,6,7,9.
The original purpose of this study was to attempt to reduce the volume of small bowel within the radiation portals during treatment of the pelvis or abdomen. We incorporated the use of a unique technique that allows the maximal displacement of the small bowel from the area of treatment using a custom made ALPHA CRADLE “BELLY BOARD” (Fig. 1).

Fig. 1 Sagittal CT showing anterior and superior abdomen displacement with patient in the Belly Board.
METHODS AND MATERIALS
PATIENT SELECTION
Thirty patients under treatment for cervical, endometrial, rectal, prostatic or bladder malignancies were studied. Seventeen patients had undergone prior pelvic surgery. Patient age ranged from 34 to 83 years and weight ranged from 110 to 260 pounds. All patients were treated to doses of 45 to 51 Gy using conventional daily fractions of 1,7 to 2.0 Gy. Some patients received another 5 to 20 Gy boost volume effectively shielding the small bowel. Patients must be able to support their own weight with their arms to make the use of an ALPHA CRADLE BELLY BOARD feasible.
CONSTRUCTION
For the study, all patients were evaluated with treatment planning CT in supine and prone positions. The patients were given both verbal and written instructions to enable reproducible bladder distension.² Patients received one liter of oral contrast 45 minutes before the scan. Anterior or posterior and lateral scanograms were obtained. CT cuts of one CM thickness were obtained for the entire length of the treatment area. Prior to the prone scan, the custom ALPHA CRADLE BELLY BOARD was fabricated.
Two or three Styrofoam® boards measuring 40 cm wide by 60 cm long by 2.5 cm thick were inserted into a large, strong plastic bag. Polyurethane mold material was mixed and added into the bag on top of the Styrofoam® sheets. The mixture was allowed to breathe adequately (approximately 45 seconds) and then the bag was securely sealed. The patient then lies on top of the bag and the mold mixture grows around the body and forms to the contours of the patient. Once the mold has hardened sufficiently (5 minutes), the patient’s xiphoid process and the superior border of the planned pelvic treatment field were identified clinically or by scanogram or fluoroscopy and these margins were marked on the patient and on the mold to assure accurate repositioning. After removing the patient from the mold, a hole was cut at the previously designated margins, leaving the lateral edges of the mold intact for increased stability (especially important for obese patients). The extracted hole usually measures 25 x 30 x 5-7.5 cm deep. All rough and exposed edges were taped for patient comfort. The patient then returned to the mold in the original position using the alignment match lines, and prone CT scan completed.
Oral contrast as described above was used for simulation of a conventional four field technique incorporating cerrobend blocking were indicated both with the patient supine and prone. The ALPHA CRADLE BELLY BOARD mold was used for the simulation in the prone position.
PLANNING AND DOSE VOLUME ANALYSIS
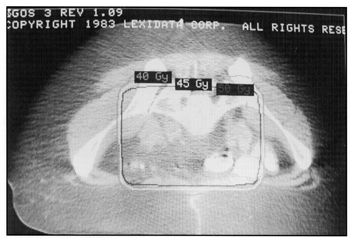
An in house image processing package was used to determine the actual volume of small bowel within the treatment areas for both supine and prone positions. The physician outlined the small bowel regions on each CT cut. Treatment fields with isodose lines incorporated were digitized from treatment plans and correlated with the CT images. All areas of small bowel within the 45 Gy isodose line were highlighted (Fig. 2). The areas were summed on each slice and the total volume of small bowel was computed by multiplying the total area by the individual slice thickness. When using the ALPHA CRADLE BELLY BOARD in the prone position, it was found that the volume of small bowel displacement increased by 66% as compared to the usual supine position. Bladder distention to S1/S2 was also routinely achieved. No patient had an increase of small bowel volume irradiated when using the ALPHA CRADLE BELLY BOARD.

Fig. 2 CT scan slice showing position of 45 GY isodose curve over outlined small bowel in prone Belly Board position.
VARIATIONS
A custom mold was also fabricated for abdominal malignancies following the same basic steps as with the ALPHA CRADLE BELLY BOARD. An extra 20 x 20 cm Styrofoam® piece was placed on top of the larger Styrofoam® sheets, on the affected side in the area of the planned radiation portal. The hole was cut to midline only from the unaffected side. This allows the small bowel to drop laterally away from the treatment field.
CONCLUSION
The use of a prone ALPHA CRADLE BELLY BOARD technique for pelvic as well as for upper abdominal malignancies, displaces, and thereby spares, as considerable amount of small bowel which reduces the gastrointestinal complications and patient discomfort. The manufacture of each custom board is a quick and simple process. The materials necessary to construct each board are easy to obtain and relatively inexpensive. The board can be formed to any shape necessary to spare the bowel or other internal structure for pelvic as well as for abdominal treatment portals. The board I fairly comfortable for the patient and increases the stability and reproducibility of treatment fields. Storage presents few problems and each mold is disposed with institutional refuse. We have investigated the attenuation factors and effects on skin sparing for various energies above 10 Mv, as previously studies.10
The ultimate goal of this project was to reduce morbidity sufficiently to allow an increase in total dose when clinically necessary. By using the prone ALPHA CRADLE BELLY BOARD technique, the small bowel no longer remains a dose limitation factor.