MINIMIZING RADIATION DOSE TO THE HEART THROUGH USE OF THE ALPHA CRADLE® IMMOBILIZATION DEVICE
John J. Smith, BA, RTT
Gary J. Schreiber, MD
St. Francis Hospital
Evanston, Illinois
INTRODUCTION
The role of radiation therapy for non-small lung cancer is controversial. Weisenberger et al1 in the randomized Lung Cancer Study Group trial noted no increase in survival but did note an increased control of intrathoracic disease for patients with Stage II or III disease. Van Houtte found a decrease in survival in patients without nodal metastasis when given post operative radiation following pneumonectomy.2 One of the arguments in favor of treating patients in the adjuvant setting is that the treatment of mediastinal recurrences is more difficult both technically as well as physically because of patient morbidity. The increased morbidity is in part related to increased volume of normal cardiac tissue incidentally included in the treatment volume. The increased volume can lead to higher risk of pericarditis and cardiac dysfunction. This case demonstrates the ALPHA CRADLE® immobilization device can be used to immobilize patients and naturally displace some of the cardiac silhouette from the treatment volume, thereby minimizing the radiation dose to the heart.
METHODS AND MATERIALS
In December of 1992 E.P. a 70 y/o female with a 25 pack year smoking history presented with wheezing and dyspnea, a CXR was obtained and confirmed the presence of an abnormal mass in the left lung. Workup revealed a squamous carcinoma of the left upper lobe. No evidence of adenopathy or distant metastasis was found, after staging with CT scans and bone scans. A complete left pneumonectomy was performed.
Mediastinal lymph node sampling was negative for spread of local disease, therefore no adjuvant therapy was indicated at that time. In July of 1993, the patient developed some hoarseness, and was seen by the ENT surgeon, who found a left true vocal cord paralysis. CAT scan of the chest was consistent with a mediastinal recurrence of her primary lung carcinoma. No other evidence of metastatic disease was noted. A CT-guided biopsy confirmed the recurrent malignancy.
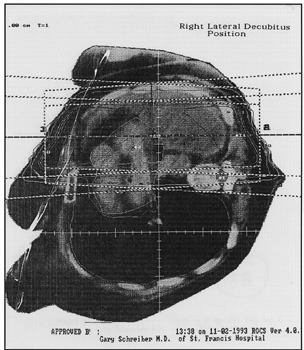
This patient’s course of radiation therapy presented somewhat of a challenge. After removal of her left lung the cardiac structures took the path of least resistance. The heart in its entirety now occupied the mid portion of the left chest cavity just behind the area of this patient’s bulky recurrent disease. A dose 4000 cGy was planned to the left hemithorax with a boost of 2000 cGy to the residual disease. A CT of the chest prior to initiation of the RT confirmed that the cardiac structures would hinder the attempt to carry the prescribe dose to eradicate her recurrent lung disease. With the risk of heart complications an alternative method of treatment was necessary. The conventional supine parallel opposed fields would require that the complete heart volume would receive the same dose as the recurrent lung tumor in the left hemithorax. A positioning alternative was then attempted. The patient was positioned in the right lateral decubitus with the hope that the cardiac structures would shift toward the mid-line thus removing a portion of the healthy cardiac structures from the target volume. With the use of an ALPHA CRADLE® immobilization and positioning device, a precise simulation was accomplished with the patient in a comfortable, secure position. The ALPHA CRADLE® form supported her shoulder, thorax and upper abdomen (Fig. 1,2). Once the simulation was complete, a CT simulation was performed with the patient in the supine position, as well as the right lateral decubitus position for comparison. As hoped, there was a significant anatomical change between the two positions. A favorable shift of the cardiac structures with the patient in the right lateral decubitus helped isolate the structures without compromising the tumor volume. Volume isodose plans were performed and confirmed that the cardiac structures would receive 25% less dose with the patient in the right lateral decubitus position (Fig. 3, 4).

Fig. 1 Patient is comfortably supported.

Fig. 2 Form Provides support while creating reproducibility.
Fig. 3

Fig. 4
DISCUSSION AND SUMMARY
Frolich3 in his discussion of radiation effects notes that cardiac radio-reactions can be transient or harmless and rarely can lead to acute left-threatening situation. However, long term morbidity from cardiac irradiation has been well documented. Radiation pericarditis and premature coronary artery disease have been described by Arsenian.4 Because significant curative therapeutic results can be obtained with radiotherapy in thoracic area and the chances for curing increase for many patients, a slight risk is justifiable for side effects on healthy adjoining tissue. On the other hand undesirable side reactions can influence the life-quality of the tumor cured patients, therefore, the aim of the radiation oncology team is to achieve uncomplicated local-regional control of cancer by radiation therapy. To accomplish this goal, precise knowledge of tumorcidal dosages and tolerance of doses of various normal tissues is most important. Unfortunately, after eight decades of radiotherapy practice, current knowledge of tolerance dose for healthy tissue an optimum curative dose for malignant tissues is still somewhat imprecise. In recent years, sophisticated treatment planning systems have been implemented. Actual CT images with the target and tumor volume superimposed with isodose curves representing the cumulative dosages of radiation to the tumor have aided in precision treatments. This advancement has resulted in major improvements to ensure adequate tumor coverage and better spacings of critical and normal structures. With the use of immobilization devices such as ALPHA CRADLE® brand Patient Repositioning Systems, positioning alternatives and treatments can be personalized under any circumstances. In this particular case the heart dose was reduced by 25% without compromising the dose to the lung tumor. It is our intention to use ALPHA CRADLE® immobilization devices on all patient procedures when a positioning variation is used.