IMMOBILIZATION AND TREATMENT OF PATIENTS RECEIVING RADIATION THERAPY FOR EXTREMITY SOFT-TISSUE SARCOMA
By Kim L. Light, RTT, CMD
Duke University Medical Center
Durham, North Carolina
INTRODUCTION
Soft-tissue sarcoma arises from mesenchymal tissue and accounts for less than 1% of cancers treated in most oncology centers. These tumors show no prevalence in any particular sex nor is there any clear age predominance, although some histologic types seem to be more common in either the younger or older patient.1
The most common site for initial presentation is the extremity. The most common presenting symptom is a painless, palpable mass.2 An effective management plan requires precise preoperative evaluation to assess the primary tumor as well as evaluation of possible metastatic disease. Conventional X-rays are useful in evaluating large tumors, although computerized tomography (CT) or magnetic resonance imaging (MRI) are considered the optimal imaging modalities in the evaluation of soft-tissue sarcomas.
Management of extremity soft-tissue sarcomas has evolved considerably over the years.2-7 It was initially thought that tumor control could be obtained with a wide local excision. Local excision alone resulted in a local recurrence rate as high as 77% in a group of 218 patients analyzed by Martin et al.7 at M.D. Anderson Hospital. Amputations at the joint above the tumor were then frequently employed to obtain clear margins. These tumors were not even considered for radiation therapy because they were considered radio resistant. Function sparing procedures that combined a more limited resection with pre- or postoperative radiation therapy are now the predominant treatment. Local recurrence rates have dropped to approximately 20% with this approach.3
With the increased use of radiation therapy for the treatment of extremity soft-tissue sarcomas, careful attention to radiation delivery is essential. Optimal precision in radiation oncology is influenced by knowledge of the dose prescribed, accurate measurements of machine output and beam parameters, as well as ensuring that the treatment beam accurately transverses the desired anatomy during every treatment. The ability to reproduce the patient position from day to day can be a major problem in radiation oncology. A reduction of as much as 10% in dose from the prescribed dose could occur if the tumor was missed due to inaccurate set up once or twice during a treatment course or if there is movement of the tumor out of the field during an individual treatment.8 Precise positioning is required to minimize this problem.
When setting up the radiation treatment fields, 5 to 10 cm margins are given longitudinally to the tumor due to its growth pattern, while a smaller margin is used circumferentially. A strip of soft tissue along the circumference of the extremity is spared to avoid edema, radiation fibrosis, and loss of function.3 A smaller margin is acceptable unless the tumor is advanced since involvement through the fascia of the muscle compartment is unlikely for localized tumors. For advanced tumors, more margin is needed and can usually be obtained with oblique fields and customized blocking to ensure some normal tissue sparing. Due to the sometimes complex field arrangement necessary for treatment of these patients, precise repositioning of the extremity is essential. A variety of immobilization techniques for other treatment sites are well described in the literature.8-16 Although it is recognized that immobilization is necessary for treating extremity sarcoma patients, there is little information in the literature detailing the positioning and immobilization technique.3,17
METHODS AND MATERIALS
Patient Positioning
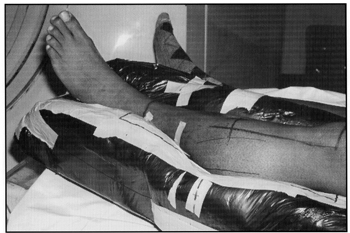
Seventy extremity soft-tissue sarcoma patients were treated with radiation therapy at our institution from 1984 to 1993. Sixty-two of these patients had sarcomas of the lower extremity and eight had sarcomas of the upper extremity. ALPHA CRADLE®* Patient Repositioning Systems were used on all patients. The location of the tumor in the affected extremity determines the position of the patient in the ALPHA CRADLE® form. Soft-tissue sarcoma occurs most often in the thigh. Tumor involvement can be extensive before a mass becomes palpable, thus large treatment volumes are usually necessary. The muscles in the thigh are divided into three groups: the anterior, medial, and posterior compartments.18 For anteriolateral tumors, treatment is usually given via parallel opposed oblique fields directed from the medial to the lateral aspect of the thigh. Anteriomedial tumors can usually be treated with AP-PA or slightly angled fields. If the tumor is proximal, the legs are separated to avoid radiation to the opposite extremity. Due to the wider field that is needed proximally, customized field shaping is used to spare normal tissue along the inferiolateral aspect of the thigh. Patients are generally positioned prone, with the involved extremity rotated, or placed on their side with their thighs separated when irradiating the posterior compartment of the thigh. At our institution, we have found that the patient’s position can best be maintained by immobilizing from the pelvis to the foot (Fig. 1).

Fig. 1 Alpha Cradle® form used when treating thigh sarcomas includes immobilization from the pelvis to the foot to ensure reproducible rotation of the extremity.
This adequately stabilizes the joint above and below the tumor site and maintains the same volume of tissue in the treatment field daily.
The muscles in the lower leg are divided into three groups: the anterior, lateral, and posterior compartments. The anterior compartment of the lower leg can be irradiated with parallel opposed oblique fields while the lateral compartment can usually be treated with an AP-PA arrangement. The posterior compartment is best treated with parallel opposed lateral fields, with the involved extremity elevated by the ALPHA CRADLE® form. The elevation of the affected leg avoids irradiation of the opposite extremity. The ALPHA CRADLE® form should include the foot and knee to avoid variable rotation of the leg from day to day.
The arm is more difficult to irradiate due to the difficulty in moving the arm far enough away from the trunk of the body. The involved muscle compartment is irradiated by rotating the arm in a position to minimize the gantry angle and spare normal tissue along the circumference of the arm. An increased gantry angle may cause the trunk of the body to be in the entrance or exit of the beam. The ALPHA CRADLE® form should include the affected arm as well as the chest and shoulders.
ALPHA CRADLE® FORM FABRICATION AND USE
The patient’s position and method of immobilization are determined prior to obtaining a treatment planning CT. ALPHA CRADLE® supplies that are needed are the foaming agents (Bottles “1” and “2”), plastic bag, protective gloves, small Styrofoam® pieces, and a large baseplate Styrofoam® piece. The patient is instructed to lie down on the baseplate in the desired position. The baseplate is cut and tailored to reflect the area being immobilized and to act as a sturdy base for the ALPHA CRADLE® foaming agents. Smaller Styrofoam® pieces are positioned and taped around the extremity as sideboards. The entire Styrofoam® Piece is inserted into the plastic bag. Usually, two-to three sets of AC325 foaming agents are used for immobilization of the lower extremity since immobilization from the pelvis to the foot is needed to ensure reproducible rotation of the extremity. When immobilizing the upper extremity, two sets of AC325 foaming agents are used. The ALPHA CRADLE® form includes the affected arm as well as the chest and shoulders. A piece of cylindrical Styrofoam® is placed in the plastic bag to form a handle for the patient to hold onto during each treatment. The immobilization of the chest and handle for the hand helps to ensure proper placement and rotation of the arm on a daily basis.
Protective gloves are worn and Bottle “1” is poured into Bottle”2” according to the instruction sheet furnished by the supplier. Bottle “2” is shaken vigorously for 10 seconds, with the cap pointing down. The mixture is poured into the bag. The bag is folded at the open end and taped with 2-inch wide tape to avoid spillage. The patient is then instructed to lie on the bag in the desired position. The small sideboard Styrofoam® pieces keep the chemicals confined to the area being immobilized. The temperature of the foam during the chemical reaction is warm and comfortable to the patient. The patient then lies motionless for about fifteen minutes while the foam solidifies. During this time, the physician comes into the CT room and marks the palpable tumor or the surgical scar with a catheter. He will also mark the approximate length of the treatment field and give instructions about the number of CT scans needed for treatment planning. Typically, the scan spacing is 1 cm through the tumor and 2 cm through the remainder of the field. The patient is aligned with the long axis of the extremity parallel to the laser and a reference catheter is placed on the line extending through the entire scan volume. The center of the scan volume is marked on the patient’s skin and the marks are extended down to both sides of the ALPHA CRADLE® form. This helps to keep the alignment of the ALPHA CRADLE® form consistent from CT to simulation. During simulation, the setup lasers and treatment fields are carefully marked on the ALPHA CRADLE® form wherever possible to ensure setup accuracy for daily treatment (Figure 2).

Fig. 2 Marks are placed on the patient and the Alpha Cradle® form to ensure set up reproducibility.
As previously mentioned, AP-PA or oblique fields are usually the best field arrangement. Oblique fields may need to be combined with wedges to minimize the dose variation within the tumor (Figure 3). The fields are routinely treated with a 4 or 6-MV photon beam. Bolus may be needed to increase the dose to the incision. No adverse reactions have been noted on the patients’ skin, even when treating through several centimeters of the ALPHA CRADLE® foam.

Fig. 3 Dose distribution for oblique wedged fields demonstrating normal tissue sparing (6 MV, 100 cm SAD, Open and 15° wedged fields).
Most patients receiving pre-operative radiation therapy at our institution for palpable tumors also receive hyperthermia and were entered onto a protocol with hyperthermia randomized to one-versus-two treatments per week.19
The ALPHA CRADLE® forms constructed for immobilization during the radiation treatment were also used on selected patients for immobilization during their hyperthermia treatment. Applicator also had an ALPHA CRADLE® constructed to create a rigid foam block to assist in positioning the applicator over the tumor area. The ALPHA CRADLE® has made the setup for subsequent hyperthermia treatments quickly reproducible and also aids in accurate replacement of thermometry sensors.20
RESULTS
All patients treated at our institution for extremity soft-tissue sarcoma in the past ten years have had ALPHA CRADLE® forms constructed for immobilization. Before 1984, a consistent treatment policy including radiation therapy was not followed. For these reasons, comparison of set-up accuracy with and without ALPHA CRADLE® forms use was not possible. Weekly approved port films and positive feedback from the technology staff, as well as the patient, demonstrates a reproducible and comfortable setup.
DISCUSSION
The optimum approach to treatment of extremity soft-tissue sarcoma involves a multidisciplinary team to determine a treatment plan for each patient. Radiation therapy combined with conservative surgery can be effective and isoptimal if tumor control and limb sparing are achieved. A good functional result is more likely to be obtained when the prescribed dose is accurately delivered. Large fields with customized blocking are often used for extremity sarcoma patients. These fields are more difficult to reproduce on a daily basis. Set-up errors can cause underdosing of the target volume or deliver dose to normal tissue not intended to be in the treatment field. All efforts should be made to improve positioning and immobilization if maximum tumor response is to be achieved.
The ALPHA CRADLE® immobilization technique described increases the comfort of the patient as well as controlling rotation of the extremity, thus improving the accuracy of the treatment delivery.